While the keto diet has exploded in popularity, there has also been an abundance of myths and misnomers about what it means to be keto. Overblown exaggerations, unfounded claims about keto being dangerous – it’s important to separate fact from fiction. In this article we will cover 11 of the biggest misconceptions about the ketogenic diet, and what the truth actually is. To cover the basics, keto is a low carb diet that is high in fat, and moderate in protein. Generally keto dieters find success with around 20 grams of carbohydrates per day, though some are able to stay in ketosis while consuming up to 50 grams of carbs daily. Since the keto diet is a fairly straightforward approach, it’s surprising that there is so much misinformation out there. So what exactly are the biggest misconceptions about the keto diet?
01. Keto is Bad for Your Health
This is perhaps one of the biggest misconceptions about keto in general. There are images of bacon, butter, and lots of other fatty foods – as if that is the ideal menu for the keto diet. The kernel of truth in this misnomer is derived from the Atkins diet – as that approach typically emphasizes foods like bacon. In reality though, a keto diet should have lots of vegetables, plenty of organic proteins, and a large amount of healthy fats (like extra virgin olive oil). In fact, the scientific data for keto dieters shows an improvement in heart health, as well as cholesterol levels. Not exactly what you’d expect from a diet that is supposedly “all about bacon and butter”. The facts could not be further from the popular misconception, in this case.
02. You’ll Have No Energy for Intense Workouts
This misnomer has a kernel of truth to it, as when performing elite anaerobic activity, there is a small decrease in performance levels. This is, of course, when compared to athletes who take in huge amounts of carbohydrates. However, for 99% of the population, your workouts are very unlikely to be impacted by keto. In fact, there are even some high-level athletes who have adopted the ketogenic diet – without any impact to their performance at all. The key is to allow for a keto adaptation period to take place. Once adapted to the keto diet, the general consensus is an improved feeling of well-being, not a decrease in performance. No truth to this misconception.
03. Keto Is Not Sustainable
This claim is perhaps the most anecdotal of all, as no scientific data backs up this statement. A ketogenic diet is very sustainable, in fact it may be the best approach for long-term weight loss, since it shifts your hormones and blood sugar into better balance. Interestingly, there is some data showing that any long-term weight loss can be difficult, but this should not come as news to those who have ever tried to lose weight. It could potentially be said that a poorly implemented keto diet is not sustainable – but no reputable source has ever recommended eating just bacon and butter. The key to a healthy keto diet is balance, so your healthy fats should be heart healthy, and your protein intake should be organic. And don’t forget non-starchy vegetables, like broccoli. Once you have established a well-rounded keto diet, it’s actually very enjoyable – and very sustainable.
04. Keto Consists Mainly of Bacon and Butter
This rumor is one of the most notorious, and again a kernel of truth leads to a statement that is wildly blown out of proportion. While you could technically eat a large amount of bacon and butter, it would not be advisable for any diet. Non-starchy veggies, well-sourced proteins, and healthy fats are the backbone of a good ketogenic diet. Bacon and butter are barely consumed, at least for most proponents of the diet. However, this reality-based explanation does not make for an interesting headline that will get clicks – so the truth goes largely unnoticed.
By this point in the article, you may see that the common theme emerging is distrust – simply because something is different. There is a little bit of a threat, whenever something comes along to challenge the status quo. The low fat, high carb diet has been entrenched in the American consciousness for about 70 years now. So anything that comes along and challenges it will automatically face some negative press attention. Unfortunately, this is the current predicament for the public perception of the keto diet.
05. You’ll Always Be Hungry on Keto
This is an interesting misnomer, as the scientific data actually shows the opposite is true. Those who consume large amounts of carbohydrates have been seen to be hungrier, less satiated, and they typically over-consume sugary foods. Lower carb dieters on the other hand, report back with higher satiety levels, less over-consumption, and more weight loss. This may be a case of just a simple viral message, as there is very little truth behind this factually challenged statement. In fact, craving some refined carbs after only a few hours of eating a muffin or donut, is far more common than being hungry on keto. Once again, the truth is actually the opposite of the public claim.
06. Keto Is Bad for Your Gut
We are not quite sure where this one came from, as the opposite has actually been found to be true. High sugar, high carb diets are closely linked with a variety of gut disorders. In fact, low carb diets are usually used in scientific studies as a way to help ease the pain of GERD, IBS, and other conditions. However, it should be noted that the gut is a very complex thing, and what’s most important is the overall microbiota population which resides in each of our individual stomachs. Taking a high-quality probiotic is still one of the best ways to repopulate your gut with good bacteria – no matter which diet you choose to follow.
07. Keto Doesn’t Work for Athletes
This misstatement is not remotely true. It’s hard to tell where this one even started. The closest truth to this statement is the adjustment period, for anyone shifting from high carb to a ketogenic approach. Many scientific studies have shown that keto actually helps with fat loss, performance, recovery, inflammation, and overall body composition. More than one study has shown lower body fat levels, increased power, and better overall performance. These benefits of course apply to athletes who follow a ketogenic diet. The truth is, athletes can be successful on many different types of diets – but again, this logical statement is unlikely to generate clicks and revenue.
08. Keto Can’t Help Diabetes
This claim may be one of the most irresponsible of all, as the opposite is actually true. Most scientific research shows that a low carbohydrate diet is the best remedy for type II diabetes. In fact, one study showed that more than half of patients reversed their diagnosis of diabetes, after just 12 months on a ketogenic diet. Nearly 100% of the participants reduced or eliminated their need for medication in the study, as well. In truth, keto diets routinely outperform diets that are specifically designed to help those with diabetes. It’s actually pretty amazing information, but for some reason falsehoods still persist.
09. Keto Makes You Feel Like You Have the Flu
This is another misconception that has a kernel of truth to it. The brief period of switching over from 200-300 grams of carbs a day, to 20 grams of carbs for keto – may cause some slight flu-like symptoms. However, not everyone experiences this, and these minor symptoms quickly pass in 3-4 days. If you do experience these symptoms, usually dehydration and/or electrolyte imbalances are to blame. So drink plenty of water, and try supplementing with electrolytes. Any ill effects should be gone almost immediately, and you’ll be well on your way to better health.
10. Keto Is Terrible For Your Heart And Cholesterol
This is another popular myth. Keto diets are high in fat – but they are healthy fats. Of course, the obvious misconception is that a keto diet is high in bad fats – therefore it must be terrible for your cholesterol and heart. Nothing could be further from the truth. In fact, keto diets help to lower bad cholesterol levels, and raise the good cholesterol in your bloodstream. Heart disease research also reflects favorably upon the keto diet. In fact, inflammation (which is the root cause of many different diseases) is usually caused by elevated blood sugar. This inflammation actually comes from a high-carb diet, not a ketogenic one. If you consume a keto diet focused around avocados, nuts and other healthy fats – you may experience even greater benefits to your health. Again, the keto diet is completely innocent of these negative health claims. In reality, keto helps your heart and cholesterol, as has been evidenced in numerous scientific studies.
11. Keto Will Make You Break Out
This claim could not be further from the truth. In fact, high sugar diets are one of the biggest culprits of acne breakouts – not low carb diets. A keto diet may actually lessen acne, as it helps to reduce inflammation, lowers IGF-1, and reduces insulin levels. Acne is closely linked with poor diet and lifestyle choices (as well as genetic factors). Besides high sugar diets, another common culprit for acne is dairy consumption. Since dairy is hugely inflammatory, as well as insulinogenic, this makes sense. Healthy fats like extra virgin olive oil, avocados, and clean proteins all aid with skin care. Of course, this middle-of-the-road analysis is unlikely to get buzz and generate clicks, even though it’s true. Once again, the truth is stranger than fiction.
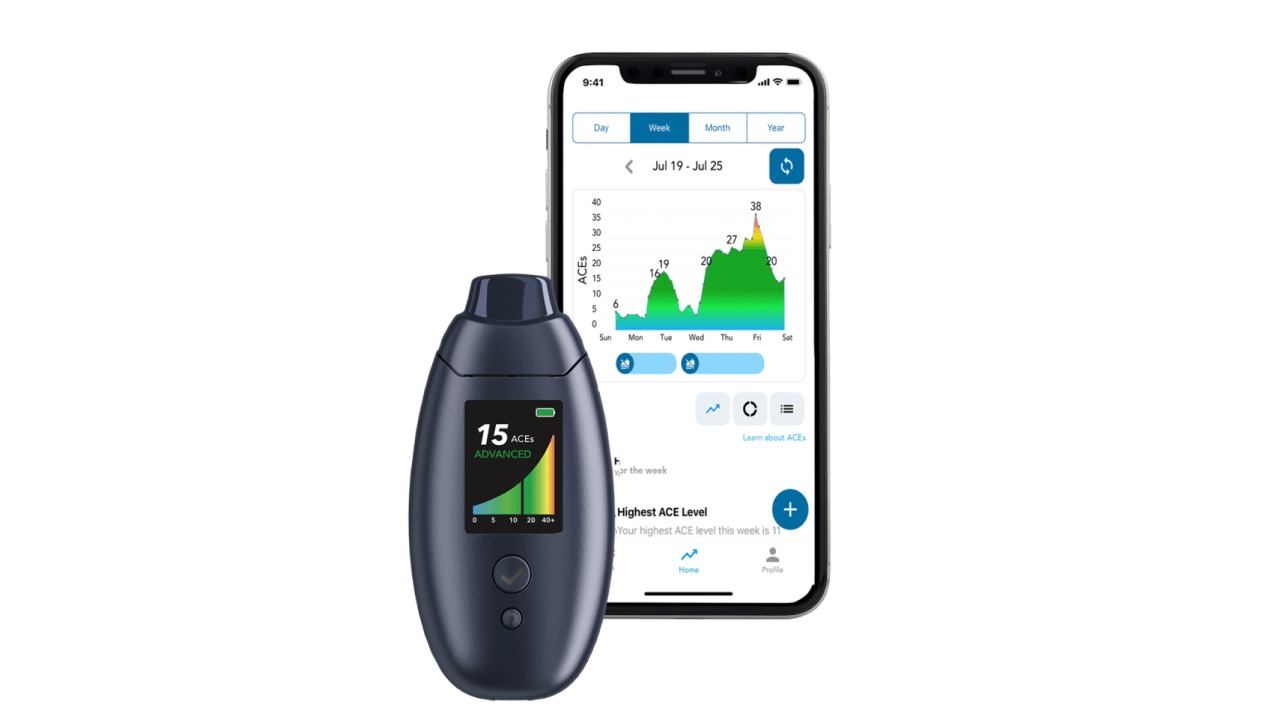
The Best Way to Measure Your Ketones
Now that you know the keto approach is actually hugely beneficial, and has little-to-no downsides, it’s time to start tracking your progress. Until now, there has not been a convenient and reliable way to check your ketones. That’s why we invented the first and only clinically backed ketone breath monitor, the first device accurate enough to replace blood measurements.. By simply breathing in our device, you will have a reliable measurement of your current ketone levels – in just seconds. No more urine strips, no more pricking your finger – just a fast, easy and reliable breath test. You can bring our device with you to the office, take it to the gym – you can truly check your ketones anywhere. Unlike previous devices, which were often poorly made, unreliable, and not backed by clinical research – our ketone breath monitor is patent pending with deep lung sampling. This means no other device is legally allowed to use our exclusive technology. Whether you are brand new to keto and want a convenient and reliable way to check your ketone levels, or you’re an elite level biohacker – we are the perfect way to measure your ketones.
You don’t need to worry about continually buying strips, or pricking your finger on a daily basis – we have all you need, in just one device. One of our favorite features is the personalized insights you get with the device. Every time you measure your ketones, your results are graphed and stored, so you can easily track your progress. Until now, there has not been an easy and convenient way to check your ketone levels – which has made many people give up on the keto diet entirely. But that outcome is no longer necessary, as we’ve made a device that does all the work for you. Just simply take one breath into the device, and within seconds you’ll know your ketone level. Whether your goal is to burn fat, lose weight, or improve your blood sugar – we have the answer.
[showhide type="references" more_text="+ Show Scientific References" less_text="- Hide Scientific References"]